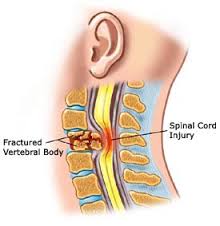
Spinal shock
During the acute phase of spinal cord we have the spinal shock, which is characterized by flaccid paralysis and abolition of the tendon reflexes and visceral, lasting from a few hours to several weeks.
In the urinary observed urinary retention, which may be up to incontinence becasuse of overflow. In this case it is recommended to deal the retention with intermittent catheterization
After restoring and leaving the spinal shock, the effects of a spinal cord injury, depending on the size of the lesion, ie if we have complete or incomplete injury, and also the size of haemorrhagic necrosis.
Damage to the sacral center and Horsetail
In this case the ejector suffers mild paralysis, taking the form of a bag that is unable to contract. Paralysis, and often involves the bladder neck, which remains open and so there incontinence.
Urodynamic observed complete absence exosfigktiriakis activit, with large bladder capacity.
Yperiera damage
In patients with damage on the spinal micturition center (I2 – I4) developed reflex detrusor activity, which characterize non anachaitizomenes contractions.
This condition is called overactive detrusor. Occurs when the detrusor reflex coexist and simultaneous contraction of the sphincter, leading to functional handicap (dyssynergia detrusor / sphincter) .
The urodynamics done after 3-6 months after the injury, when fully installed the micturition reflex and usually presents hyperreflexia detrusor dyssynergia anddetrusor / sphincter.
The patient has urinary incontinence, urinary tract infections, hydronephrosis and gritty.
In therapeutic approach, have an important place clean intermittent aftokathetiriasmoi, combined with anticholinergics to suppress reflex detrusor contractions.